
Understanding home visit demand and activity in General Practice
Kirriemuir Medical Practice
Like many other practices, Kirriemuir Medical Practice in NHS Tayside is seeing an increasing number of elderly and frail patients who generally prefer care closer to home. Within this population, patients are more likely to require urgent care delivered in their own homes.
Additionally, NHS Tayside are looking ahead to NHS Scotland’s Redesign of Urgent Care (RUC) and the Scottish General Medical Services (GMS) contract, so the practice hopes to support an overarching strategy for managing primary urgent care that will align with these frameworks.
For these reasons, the practice team wanted to obtain a clear picture of demand and activity related to home visits, including how many visits were being requested and completed, which staff members were completing them, and some outcomes of those visits. They also wanted to be able to track the impact of any changes made to home visit processes, such as changing the process of home visiting allocation or adding a new staff member.
Developing a tool and collecting data
In order to capture a comprehensive view of home visit demand and activity, two excel spreadsheets were created. One was designed to capture home visit demand, and included the following categories:
- Total number of requests from patients
- Total number of patients offered an alternative by administrative staff
- Total number added to the duty request list for clinician review
- Total additional number generated by the practice by any other means
- Total number of home visits completed on each day

Data presented is fictional and does not represent practice data
This sheet also includes a column to display the percentage of patients who were offered an appointment. Six months of baseline data was recorded before any changes were implemented.
In order to capture the outcomes of home visits, the second spreadsheet was used to record the following data about every completed home visit:
- The job role of the person who completed the visit (General Practitioner or Trainee, Advanced Nurse Practitioner, or District Nurse)
- Was an acute prescription written for the patient during the visit?
- Was the patient admitted to hospital within 72 hours of the home visit?
- Did the patient initiate contact with a GP or Out of Hours within 48 hours of the home visit?
This data was collected retrospectively by one practice GP, who did so by looking through the notes of every home visit patient from the last six months. The GP found this process quick and easy, and was able to review three months’ worth of notes, around 250 patients, in about two hours. This gave a meaningful baseline, taking normal variations into account. Note that this tool does not require six months’ worth of data to function. It will still provide a useful snapshot of activity with a smaller amount of data.
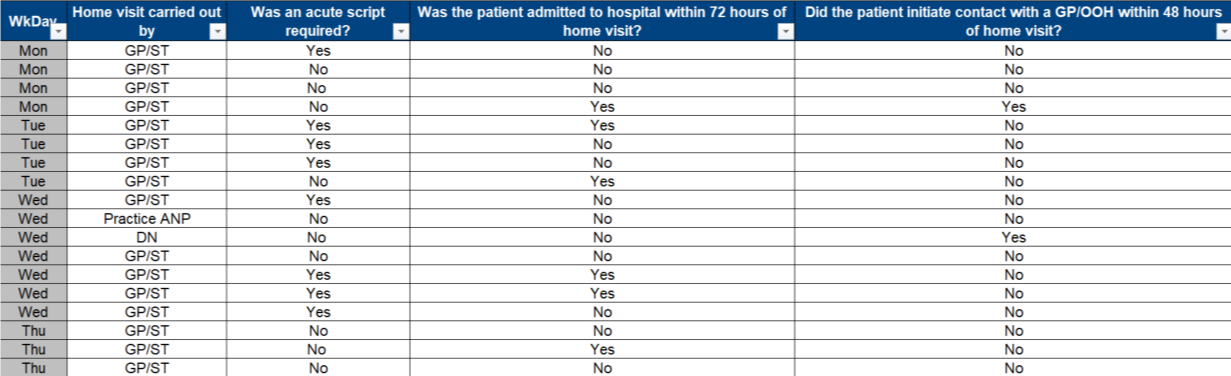
Data presented is fictional and does not represent practice data
Visualising the data
Once the data had been collected and entered into Excel, it was used to create an interactive data explorer with multiple graphs and charts showing different trends in the data. On the left side of the data explorer, there is a C-chart, a type of Statistical Process Control (SPC) chart, showing the total number of home visits completed. Below this, another chart shows the average number of home visit requests, home visits allocated, and number generated by the practice for each day of the week over the testing period. Together these can give some idea of how capacity for home visits can be planned over the working week.
In the centre of the explorer, a run chart shows the percentage of visits carried out by each staff group. Above it, a bar chart breaks down the three categories of home visit outcomes (was a prescription written, did the patient have GP contact after the visit, was the patient admitted to hospital after the visit), with percentages of patients who were either a yes or no to each of those three questions. A dropdown menu allows the user to view these percentages for visits completed by each staff group individually.
On the right side of the explorer, three more run charts show the percentages of patients requiring prescriptions, patients having GP contact, and patients admitted to hospital, used as balancing measures to check for unintended consequences.
A separate tab of the spreadsheet lets the user add annotations to the charts to show when a particular intervention has been made, such as a new staff member beginning or a change in the number of home visit slots available. This makes it possible to view and analyse the impact of an intervention.
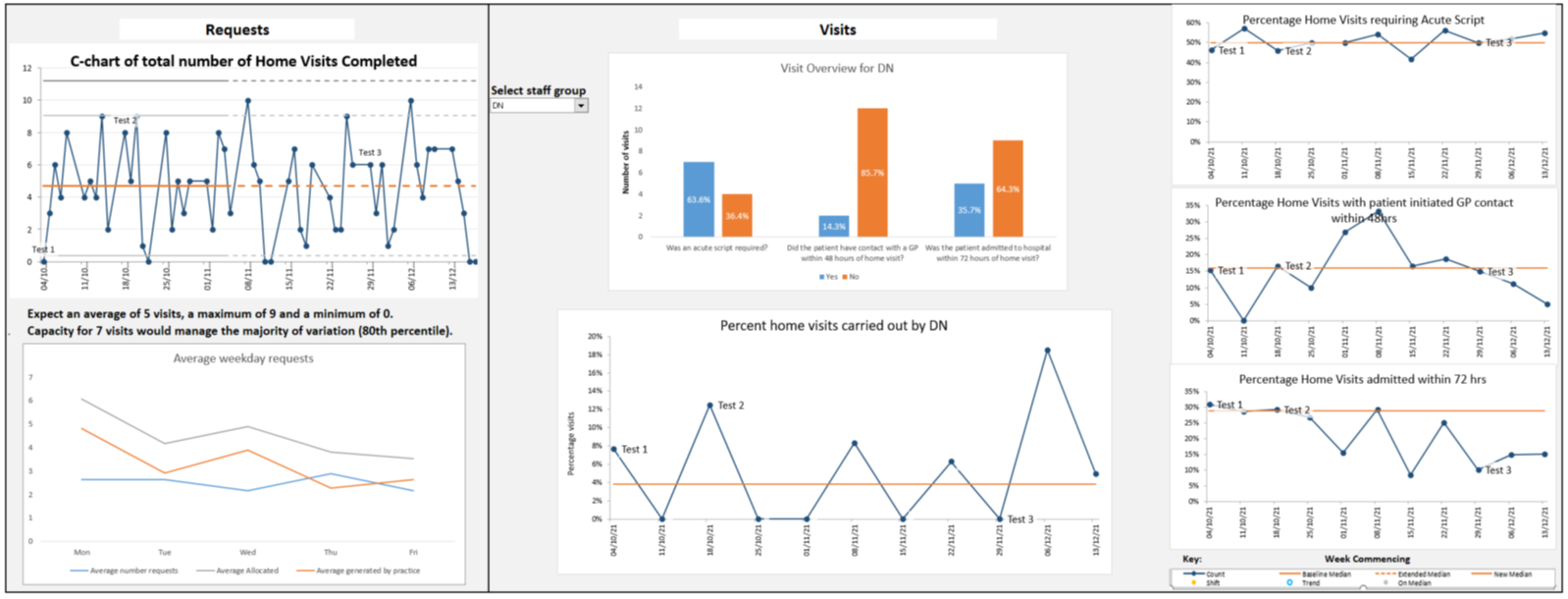
Data presented is fictional and does not represent practice data
Next steps
This data collection exercise has given the practice a comprehensive overview of home visit activity that they did not have before. The tool provides a useful starting point to explore the impact of new staff, training delivered, or process changes, and also to find the right number of appointment slots needed to effectively manage home visit demand. The practice team plans to test a number of interventions and use the tool to evaluate their impact. The data collection also demonstrated that the number of prescriptions issued and patients admitted varies for different staff groups. As such, the practice will look further into why this might be happening.
This exercise has helped us have clarity in our data that wouldn’t have been possible in any other way." General Practitioner
We would never have known how many acute prescriptions we get, we didn’t know the percentage of admissions [to hospital]… the tool lets us see what those results are." General Practitioner
It will also aid the practice and NHS Tayside in their discussions around the Redesign of Urgent Care and the GMS contract, as it can be used to provide evidence for or against particular approaches to urgent care design.
Now we’ll do more interventions, and the tool will help us show how effective those interventions have been." General Practitioner
Click here to access the home visit explorer, which can be customised to meet your practice requirements.